
Menopause How We Need To Understand It And What Can Be Done (part 1)
- 12 minutes ago
- 5 min read
#Tejasvani knowledge desk
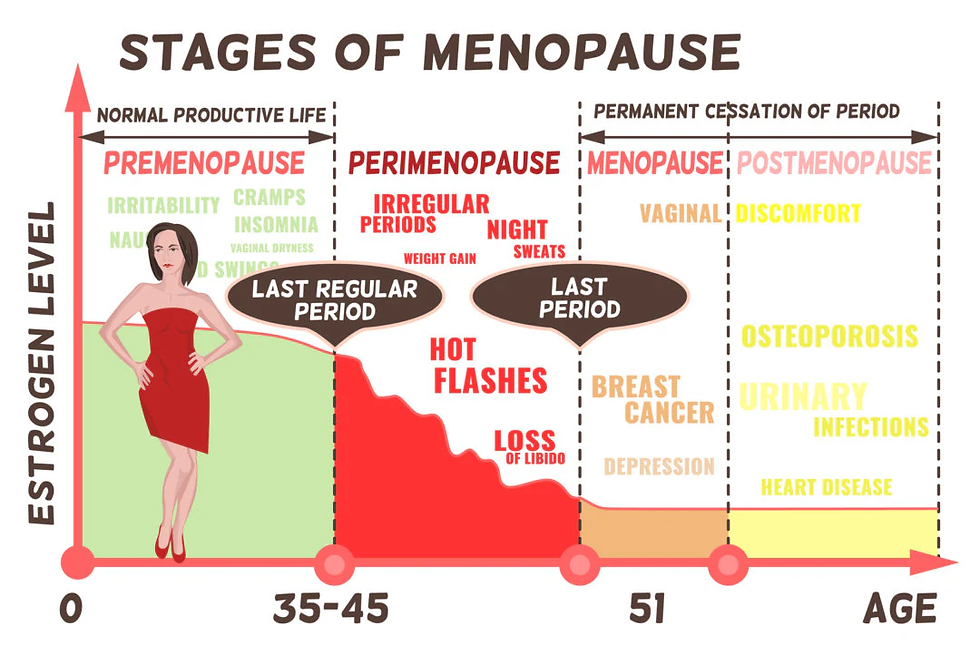
Typically, between the ages of 45 and 52 years, women inevitably go through menopause and hormonal changes, and the absence of menstruation is its defining characteristic. In most cases, menopause begins in women at 42 years of age. Perimenopause is a transition period that begins several years before menstruation and is marked by the cessation of more significant functions. Hot flashes, nocturnal sweats, and psychosomatic symptoms are all part of acute menopausal syndrome, which is classified on a scale of 1–4, including depressive symptoms, attention-deficient disorder, pain in the bones and joints, migraines, arrhythmias, and para-anesthesia

The best treatment marketed is hormone therapy. The use of hormone treatment has declined in recent decades. The Women’s Health Initiative found that hormone therapy is associated with a higher risk of breast cancer and cardiovascular disease. Nonhormonal medications: Paroxetine/ Fezolinetant both FDA approved thought the latter carries a box warning toxic to liver while first one is weak in impact and both operate by rupturing signaling ways, which is recognized to be bad and hence what we are left is with not much.

Menopause represents the natural and permanent cessation of menstruation resulting from declining ovarian function and estrogen deficiency. The term signifying the end of the reproductive years is defined as 12 months of amenorrhea. Natural menopause most commonly occurs between ages 45 and 56, with a median age of 51 in the United States.
Advancing age leads to progressive depletion of ovarian follicles through atresia and ovulation. Granulosa cell numbers within the ovary decline, reducing production of estradiol and inhibin B. Levels of antimullerian hormone (AMH), another hormone secreted by ovarian granulosa cells, also decrease. Reduced inhibitory feedback from estrogen and inhibin A and B results in increased production of follicle-stimulating hormone (FSH) and luteinizing hormone (LH). Declining estrogen levels disrupt the hypothalamic-pituitary-ovarian axis and impair normal endometrial development. These hormonal and physiologic changes contribute to irregular menstrual cycles that ultimately progress to complete cessation of menses.
During the perimenopausal period, the earliest menstrual change commonly involves shortening of the follicular phase, which leads to more frequent menses. Subsequent progression usually produces longer menstrual cycles. Many cycles become anovulatory, resulting in perimenopausal abnormal uterine bleeding. Menstruation eventually ceases completely. Testosterone levels change minimally during early menopause, creating a relative increase in the testosterone-to-estrogen ratio that may produce symptoms associated with androgen excess.
Menopause may also result from surgical procedures.
Urogenital changes occur during menopause as declining estrogen levels affect vulvar and vaginal tissues. Inflammation of mucosal surfaces develops, producing erythema and increased tissue friability. Vaginal pH rises, and parabasal cell populations increase. Structural alterations also occur, including narrowing of the introitus, thinning of the labia, and reductions in both vaginal depth and width.
Vasomotor Symptoms
Vasomotor symptoms represent the most common manifestations during the menopausal transition. Approximately 75% to 80% of women experience these symptoms with varying severity. Common manifestations include hot flashes, night sweats, palpitations, and migraines. Hot flashes occur unpredictably during both daytime and nighttime and typically last about 3 to 4 minutes. Each episode begins with a sensation of flushing that spreads across the upper body, reflecting central nervous system alterations in thermoregulation. Such episodes may disrupt daily activities and impair sleep quality. Vasomotor symptoms persist for an average duration of 1 to 6 years and continue for as long as 15 years in 10% to 15% of postmenopausal women. Alcohol consumption, smoking, obesity, physical inactivity, and emotional stress may worsen symptom severity.

Hot flashes
Hot flash is the term used to describe a sudden and intense sensation of heat mainly involving the upper body, typically the chest, neck, and face. Hot flashes typically only last one to five minutes but can happen anywhere from one to 10 or more times a day. They may also be accompanied by clammy or flushed skin, a sense of anxiety, a fluttery or fast heartbeat, and sweating. The sudden wave of heat is often followed by chills, which can be equally—if not more bothersome than the flash of heat and sweating.

The underlying causes and triggers of hot flashes are not completely understood, but we know that the hormone estrogen is relevant. The fluctuations in estrogen levels in perimenopause and the loss of ovarian estrogen at menopause play a role.
Declining estrogen levels, which disrupt the brain's internal thermostat (the hypothalamus). When this occurs, the brain overreacts to minor temperature shifts, triggering sudden, intense waves of heat, sweating, and flushing as the body attempts to cool itself down.
Dropping estrogen levels hyper-stimulates specific nerve cells (called KNDy neurons) in the hypothalamus. This misfires a "you are too hot" signal to the body
To lower what it incorrectly perceives as an overheating threat, brain initiates a massive cooling chain reaction. Blood vessels rapidly dilate to push blood to the surface of the skin (causing redness and flushing) and sweat glands activate to release heat, if any of these mechanisms aimed at heat loss overshoot, it leads to a transient drop in inner body temperature, triggering shivers in an attempt to retain heat, there may also be a temporary increase in heart rate as part of the body's effort to dissipate and retain heat.
Migraine patterns may change during the menopausal transition
Migraines represent neurovascular headaches frequently triggered by fluctuations in estrogen levels. Early menopausal hormonal variability may worsen migraine severity or frequency. Many women experience migraine improvement after menopause, although some report worsening symptoms. Migraine with aura carries an increased risk of stroke, particularly among individuals who smoke or use oral contraceptives. Other headache types, including cluster headaches and tension headaches, may also increase with hormonal fluctuations.

Genitourinary Symptoms
Genitourinary syndrome of menopause affects approximately 50% to 75% of women. Thinning of the vaginal mucosa and reduced vaginal elasticity develop as estrogen levels decline. These physiologic changes may produce vaginal dryness, burning, pruritus, and irritation. Urinary symptoms, eg, frequency and urgency, frequently occur because estrogen receptors exist within the bladder and urethra. Urethral atrophy may lead to frequency, urgency, and dysuria. Reduced estrogen levels may also increase the risk of recurrent urinary tract infections. Elevated vaginal pH promotes bacterial colonization of the vagina by bladder pathogens.

Psychogenic Symptoms
Psychogenic symptoms occur in up to 70% of women during perimenopause and menopause. Common manifestations include anger or irritability, anxiety or tension, depression, impaired concentration, and reduced self-esteem or confidence. Sleep apnea, insomnia, and restless legs syndrome may contribute to sleep disturbances beyond those associated with night sweats. Estrogen receptors are present in multiple brain regions involved in mood and cognitive regulation. Declining estrogen levels, therefore, influence emotional regulation.
Estrogen also modulates serotonin and noradrenaline transmission, which supports mood stability. Some mood changes may reflect evolving personal or social circumstances rather than hormonal influences alone. Perimenopausal women demonstrate a higher risk of depressive symptoms and greater symptom severity compared with premenopausal women. Vasomotor symptoms and additional factors that remain incompletely defined may contribute to this increased risk of depression during perimenopause and menopause.
STRAW +10 staging system is considered to be golden standard to measure this cycle. Long-term complications of menopause are largely linked to decreased estrogen levels, with cardiovascular disease and osteoporosis representing the most significant health concerns.
Part 2 will evaluate herbs that have been historically used and current clinical researches on them. We have to understand we as humans are 10000-year-old while as formal medicines are only 150-year-old history and even today majority of treatments comes from herbs be it ayurveda of 3000 years, Chinese with 2000 years, unani with 1800 years or homeopathy with 350 years



Comments