
Menopause Weight Gain In Asian Women And What We Can Do
- Jun 6
- 6 min read
Midlife weight gain is primarily driven by aging, reduced metabolic rates, and lifestyle changes, rather than hormonal shifts alone. However, dropping estrogen levels significantly trigger a shift from "pear-shaped" (gluteal-femoral) to "apple-shaped" (abdominal) fat deposition, escalating cardiometabolic risks.

Asian women tend to accumulate more visceral (abdominal) fat than Caucasian women of a comparable Body Mass Index (BMI). As ovarian function declines, the decrease in estrogen leads to a shift in fat distribution toward the visceral/abdominal region, increasing the risk of metabolic syndrome and cardiovascular disease. Midlife is accompanied by a natural loss of muscle mass (sarcopenia) and a declining BMR. If women maintain the same caloric intake as in their younger years, weight gain is inevitable. Rapid modernization and urbanization in regions like India have shifted dietary habits and reduced physical activity levels.
The age at which menopause occurs is influenced by a combination of genetic, environmental, and lifestyle factors. It serves as an important indicator of ovarian reserve and overall reproductive aging. Early menopause, defined as occurring before the age of 40, may be associated with increased risks of cardiovascular diseases, osteoporosis, and mortality, whereas later menopause may heighten the risk of breast and endometrial cancers.
“Studies from India, Pakistan, and to some extent Sri Lanka, reported lower menopause ages with mean ages at or below 46.37 years. The earliest average menopausal age was 44.5 years, reported by Adhi et al. in Pakistan. Relatively earlier mean age of menopause was also reported in India, with estimates ranging from 44.92 to 47.9 years, and several studies clustered around 46.2 years. Studies by Dasgupta and Ray observed a significant rural–urban gap, with urban women reaching menopausal age nearly 2 years earlier than their rural counterparts. (Prabhat Kumar Agrawal et al 205) against western average above 50.

“In Asian countries, postmenopausal women often report higher incidences of backaches and muscle, shoulder and joint pain, but fewer vasomotor symptoms (VMS) disturbances compared with their counterparts in Western countries. The exact reasons for these discrepancies remain elusive but may be related to lower estrogen levels with menopausal transition, which may drive greater SCI. In fact, the Study of Women’s Health Across the Nation (SWAN) in the USA reported lower estradiol levels during midlife in Chinese and Japanese women compared with Caucasian and African American women. Additionally, specific dietary patterns and cultural factors in certain Asian regions are linked to high prevalence of deficiencies in vitamin B12 [, vitamin D, vitamin C, calcium, iron and zinc. A review on micronutrient needs of aging populations in the Asia-Pacific identified vitamins A, D, E, C and B12, zinc and omega-3 fatty acids as particularly important. (Unnop Jaisamrarn et al 2025)
For women in early midlife, the interplay between chronological aging and ovarian aging significantly impacts overall health and quality of life. While symptoms resulting from estrogen decline are prominent during this stage of life, the impact of underlying health conditions may be more subtle and not immediately apparent. The expert panel advocates for women and healthcare professionals (HCPs) to approach health challenges in midlife and the menopausal transition holistically.
In April 2024, a panel from eight countries/regions in the Asia-Pacific – representing endocrinology, gynaecology, nutrition, psychiatry, orthopaedics, lifestyle medicine and primary care – convened to deliberate key health issues affecting women in early midlife and during the menopausal transition. The panel identified an interplay between hormonal fluctuations, SCI and micronutrient deficiencies as a unifying concept, with dysfunctions in these areas contributing to menopausal symptoms, metabolic syndrome (MetS), impaired mobility and neurocognitive changes and provided a pyramid structure to be considered holistically.
Hormonal fluctuations lead to menopause-specific symptoms such as VMS (vasomotor symptoms—the medical term for hot flashes and night sweats. They are the hallmark symptoms of menopause, caused by fluctuating estrogen levels that disrupt the body's internal temperature control. VMS affects up to 80% of women during the menopausal transition and can persist for years. which affect 34.5–61.0% of women in Asia and persist for a median duration of 10.2 years. VMS contributes to other health conditions such as sleep difficulty, anxiety and depression. Estrogen decline also reduces energy expenditure and physical activity, leading to weight gain. At the same time, changes in follicle stimulating hormone and androgen-to-estrogen ratios promote fat accumulation and increased body mass index. SCI (spinal cord injury), which develops with aging, leads to progressive tissue damage and is further exacerbated by the decline in anti-inflammatory effects as ovarian steroidal hormones diminish during the menopausal transition. Micronutrient deficiencies further compound these challenges. A systematic review of 90 studies found that postmenopausal women with deficiencies in nutrients like vitamin B6, vitamin B12, vitamin D, iron, omega-3 fatty acids and lycopene are at a higher risk for cardiovascular and cerebrovascular events, metabolic disorders, osteoporosis, obesity, cancer, neurodegenerative conditions, depression, cognitive decline and dementia. During the menopausal transition, deficiencies in key nutrients, such as calcium and vitamin D, are common, as estrogen aids calcium absorption and vitamin D activation. SCI conditions also reduce the absorption of calcium, vitamin D, the vitamin B group, iron, vitamin A and zinc. Additionally, chronic diseases can impact iron metabolism, with iron-deficiency anaemia affecting 30–60% of perimenopausal women. Conversely, deficiencies in nutrients such as iron, vitamin B6 and vitamin A may elevate pro-inflammatory markers.

Low-grade SCI can induce neuroinflammation, which leads to alterations in brain structure and neurochemical processes. This, coupled with the decline of estrogen, which helps maintain neuronal activity and neurogenesis, contributes to neuropsychological and cognitive decline, as well as increased susceptibility to mood disorders. Psychological distress, including depression and anxiety, can be intensified by VMS. Additionally, deficiencies in protein, vitamins B and D, magnesium, zinc, selenium, iron, calcium and omega-3 fatty acids have been reported to impact the brain and nervous system adversely, with many of these deficiencies further exacerbated by aging and estrogen decline during menopause.
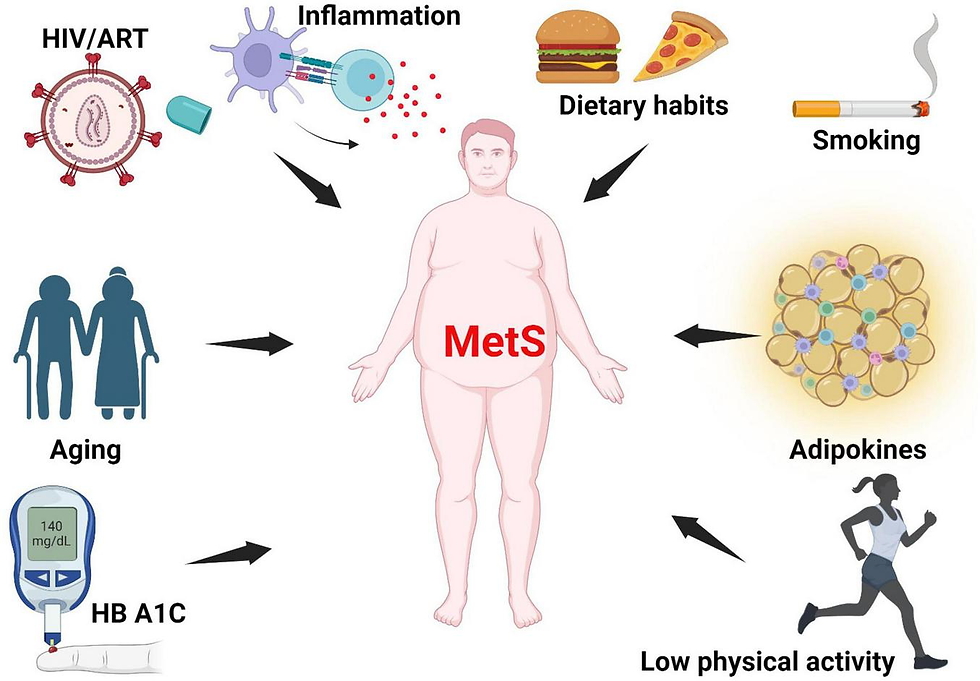
MetS, marked by central obesity, insulin resistance, dyslipidemia and hypertension, becomes more prevalent with aging and often accompanies low-grade SCI Menopause and estrogen decline are linked to increased rates of MetS and related conditions, with studies showing increased abdominal obesity, triglycerides, total cholesterol, low-density lipoprotein cholesterol, fasting glucose, insulin resistance, body mass index and blood pressure. Deficiencies in vitamin D, magnesium, vitamin E and B-group vitamins are associated with an increased risk of MetS, and levels of these micronutrients appear to decline with aging and during the menopausal transition.
Medicinal plants as a potential source of phytoestrogens
Phytoestrogens are a diverse group of non-steroidal compounds of plant origin or biologically derived from plant precursors, are structurally similar to the primary female sex hormone, E2 (Yokosuka et al., 2021). Four phenolic compounds identified as phytoestrogens are isoflavones, stilbenes, coumestans, and lignans. They are found in a wide array of plants, primarily categorized into these four classes (Desmawati and Sulastri, 2019). Major sources of isoflavones include legumes such as Glycine max (L.) Merr. (soy) and its products, Trifolium pratense L. (TP, red clover), and NS (black cumin), while fiber-rich foods such as unrefined grains, cereal brans, and beans are abundant in lignans (Bedell et al., 2014). The most studied isoflavones, including genistein, daidzein, glycitein, formononetin, and biochanin A, are prevalent in soybeans. Although a diet low in phytoestrogens does not lead to any deficiency syndrome, given their structural resemblance to synthetic estrogen and their ability to bind to estrogen receptors, they hold therapeutic significance (Rietjens et al., 2017).

Phytoestrogens act as mild estrogen agonists that target certain receptors and cell types via ERα, ERβ, and other signaling pathways. Thus, with estrogen-like effects, phytoestrogens increase estrogen levels in the body and provide post-menopausal women with a practical alternative to synthetic HRT, which has certain side effects. Plant-based estrogen can reduce the risk of clotting and alleviate menopausal symptoms like hot flashes and osteoporosis, and many women have begun to use phytoestrogen supplements (Franco et al., 2016). Furthermore, exposure to phytoestrogens can reduce the risks of cardiovascular disease, obesity, MetS, type 2 diabetes mellitus, brain function disorders, breast cancer, and other malignancies, including prostate and colorectal cancers. However, the potential hormonerelated side effects of phytoestrogen treatment, such as endometrial hyperplasia,endometrial cancer, and breast cancer, remain uncertain. Consequently, the safety and tolerance of long-term supplementation with phytoestrogens are under scrutiny. Additionally, other phytochemicals, such as triterpenoids, phenols, flavonoids, lignans, sterols, terpenoids, iridoids, polysaccharides, amino acids, unsaturated FAs, carbohydrates, and carotene, were found in Lycium chinense Mill. (LC), Ocimum gratissimum L. (OG), Eucommia ulmoides Oliv. (EU), Pueraria lobata (Willd.) Ohwi (PL), Rehmannia glutinosa (Gaertn.) DC. (RG), Cornus officinalis Siebold & Zucc. (CO), and Daucus carota L. (DC). These phytochemicals render the above plants pharmacologically important for treating various severe illnesses, including cancer.
A kit can be made and it looks we will need to incorporate healers who are already dealing with nutrition especially micro nutrients. Increase soya use must be ideally with one from mountains known to be organic and we are coming with soya bean based probiotic from Manipur shortly.





Comments